Whiplash, Neuroinflammation, and Neural Edema: Why Sports Medicine Is Finally Catching Up
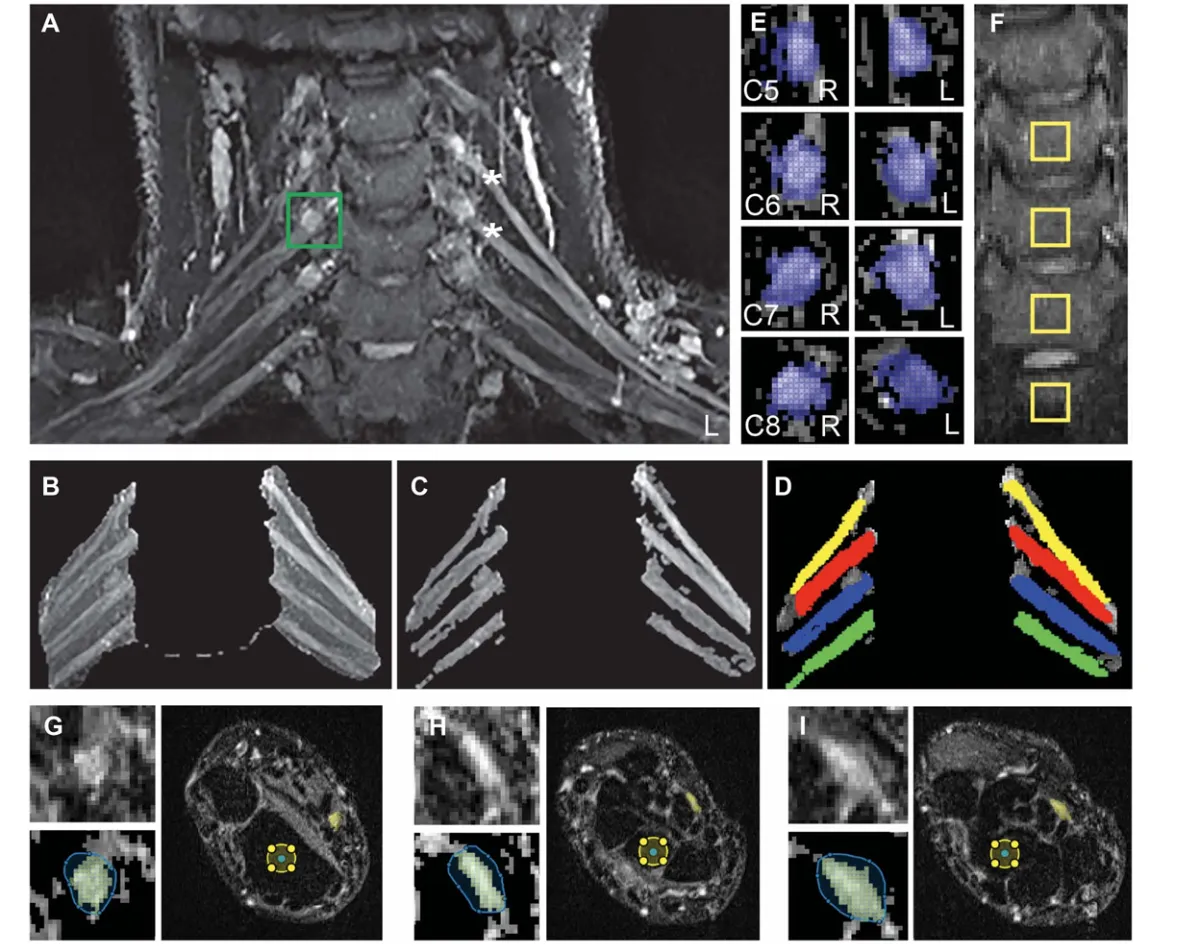
figure: ImageanalysisofT2weightedimagesofthebrachialplexus,dorsalrootganglia(DRG),andmediannerveatthewrist.(A)ExampleT2maximumintensity projection image formed from extracted selected slices. A bounding box is shown positioned around the right C6 DRG (green square). (B) Freehand mask drawn aroundtherootsoftheplexusonthemaximumintensityprojectionimage.(C)Segmentedregionsoverlaidtoproduceacompletesegmentedimageoftherootsof the brachial plexus. (D) Regions of interest overlaid on C5 to C8 roots. (E) Bounding boxes positioned around the C5-C8 DRG. (F) C5 to T1 vertebral bodies showingthe4controlROIs(10310voxels).(G–I)Exampleaxialslicesofthemediannerveatthewrist,atthe(G)distalradioulnarjoint,(H)proximalcarpalrow,and (I) distal carpal row. Upper left of (G–I): Enlarged image of the median nerve. Lower left of (G–I): Freehand mask drawn around nerve and segmented median nerve (yellow). Right of (G–I): Complete axial slice across wrist showing the segmented median nerve (yellow) and the control region of interest in the underlying bone (yellow circle). The T2-weighted scans were from WADII participants. Note the brighter C5 and C6 roots of the brachial plexus on the left side (*), which corresponded to the most symptomatic side in this participant. ROI, regions of interest; WADII, whiplash-associated disorder grade II
Every now and then a paper comes along that does not feel surprising.
It feels confirming.
That is exactly how I felt reading the recent paper on peripheral neuroinflammation after acute whiplash. For many clinicians, this may sound like an emerging topic. For me, it feels more like the research is finally catching up with something I, and my mentor Dr. Alejandro Elorriaga, have been teaching for years through the Contemporary Medical Acupuncture Program at McMaster University.
And that matters.
Because for a long time, many of us working clinically have seen patients whose presentation did not fit neatly into a simple tissue-based model. They were not behaving like a straightforward muscle strain. They were not progressing like a routine joint irritation. Their symptoms had a neural quality to them. The mechanosensitivity was there. The sensory changes were there. The irritability was there. But the research language around it was still developing.
Now that picture is becoming clearer.
New research on whiplash and peripheral neuroinflammation
This recent paper looked at people with acute whiplash-associated disorder grade II, or acute WADII, within four weeks of injury. Traditionally, WADII has been classified as neck pain with musculoskeletal signs but without clear neurological signs. That definition has shaped how many clinicians think about whiplash cases. This study challenges that model directly.
The researchers found evidence suggesting that a subgroup of these patients had signs consistent with peripheral neuroinflammation. They reported increased MRI T2 signal in the C5 root of the brachial plexus and the C5-C8 dorsal root ganglia, findings consistent with intraneural oedema associated with neuroinflammation. They also found that 55% of participants had signs of heightened nerve mechanosensitivity, 47% had somatosensory changes, and inflammatory mediators including IFN-g, IL-6, and IL-8 were elevated compared with healthy controls.
That is not a small clinical observation.
That is a meaningful shift in how we may need to understand some post-whiplash presentations.
Why this research feels familiar
For me, this is less about discovering something brand new and more about seeing an important idea formally enter the literature.
For years, this has been part of the clinical conversation in the circles I learned from and taught within. Dr. Alejandro Elorriaga has been teaching these ideas for a long time. In the Contemporary Medical Acupuncture Program at McMaster University, this was never just an abstract theory. It was part of how we worked to understand the patient in front of us with more precision.
What are we really looking at here.
Is this only a local tissue problem.
Or are we dealing with neural tissue that has become sensitized, irritated, inflamed, mechanically reactive, or functionally altered in a way that changes the entire presentation.
That distinction matters because it changes assessment.
And when assessment changes, management changes.
Neural edema and whiplash are not new ideas
I also want to point out that this is not the first time I have written on this topic.
About two years ago, I wrote a blog on neural edema and its clinical relevance. At the time, this was not a mainstream topic in sports medicine, but clinically it already felt important. This new paper gives more structure, more imaging support, and more research language to a conversation that many experienced clinicians have already been having.
You can read that earlier piece here: https://skillsinhand.com/post/intraneuraledema
That earlier article and this new research fit together well. The older blog addressed the clinical idea. This newer paper gives us more evidence for why that idea deserves more attention.
Why sports medicine is finally paying attention
This is the bigger story.
Sports medicine has often been very strong in tissue-based reasoning, exercise prescription, rehab progressions, and load management. Those are valuable tools. But there are cases where they do not fully explain what is happening. Some patients do not respond the way a purely nociceptive model would predict. They remain highly irritable. Their symptoms spread or fluctuate. Their response to movement, tension, compression, or loading does not behave like a straightforward contractile or articular problem.
That is where clinicians often get stuck.
This paper helps explain why.
The authors state that their findings are in direct contradiction to the traditional Quebec criteria for WADII and suggest that whiplash diagnostic grades may need revising to include sensory changes consistent with peripheral neuroinflammation and tests for heightened nerve mechanosensitivity. They also note that current management may need reconsideration when minor peripheral nerve injury is present.
That is a significant statement.
And it should get the attention of clinicians working in sports medicine, rehab, and pain care.
Why nervous system assessment matters in whiplash
One of the most useful takeaways from this paper is not just that neuroinflammation may be present.
It is that better nervous system assessment matters.
The study found reduced elbow ROM during ULNT1, more local or referred pain with brachial plexus palpation, elevated inflammatory markers, and meaningful sensory changes in a substantial subgroup of patients. It also found that clinicians should be mindful of nerve involvement and include detailed neurological screening and tests for heightened nerve mechanosensitivity.
This is where clinical reasoning really earns its keep.
If you do not assess the nervous system properly, you may misclassify the problem.
If you misclassify the problem, you may choose the wrong management strategy.
And if that happens, it is no surprise when outcomes stall.
The paper also points out that when neuroinflammatory or neuropathic features are present, management may need to look different from a standard nociceptive pathway. The authors mention possibilities such as neuropathic-pain-oriented pharmacology, therapies targeting neuroinflammation, and conservative strategies such as neurodynamic interventions.
Again, that is not a minor detail.
Classification drives treatment.
Research usually arrives after clinical reality
This is something I have seen again and again.
First, good clinicians notice patterns.
Then they refine those patterns through experience.
Then they teach them.
Only later does the research start to organize and validate what was already visible in practice.
That is what this moment feels like to me.
Not the arrival of a completely new idea.
More like the formal recognition of something that has been clinically relevant for years.
And that is good for the profession, because once the literature starts moving, the wider clinical conversation often moves with it.
Final thoughts on whiplash, neuroinflammation, and clinical practice
I am glad to see whiplash neuroinflammation becoming part of the research conversation in a more visible way.
Not because one paper settles everything.
It does not.
But because it pushes the profession toward a more complete view of pain, trauma, and the nervous system. It supports the idea that some patients need more than a standard tissue-based lens. It gives more credibility to the kind of clinical reasoning that looks carefully at mechanosensitivity, sensory change, neural edema, and nerve involvement. And it reinforces something that has been taught for years by clinicians like Dr. Alejandro Elorriaga in the Contemporary Medical Acupuncture Program at McMaster University.
For those of us who have been paying attention to this for a long time, it is good to see the research finally entering the picture.
If you want to explore this clinical way of thinking more deeply, take a look at the Contemporary Medical Acupuncture Program at McMaster University.
https://mcmasteracupuncture.com/
And if you want more context, I also recommend reading my earlier piece on neural edema here:
https://skillsinhand.com/post/intraneuraledema
As I always say, knowledge is value.
The better you understand what you are actually seeing, the better decisions you may make for your patients.

